Isolated Bilateral Lateral Geniculate Body Necrosis Following Acute Pancreatitis
A Rare Cause of Sudden Bilateral Vision Loss in a 20-Year-Old Male
________________________________________
Clinical Presentation:
A 20-year-old male presented with acute, painless bilateral vision loss during recovery from acute necrotizing pancreatitis. There was no history of trauma, seizure, or metabolic disorder. Visual evoked potentials were absent bilaterally. Pupillary reflexes were intact. Fundus and optic nerve evaluations were unremarkable.
________________________________________
MRI Findings:
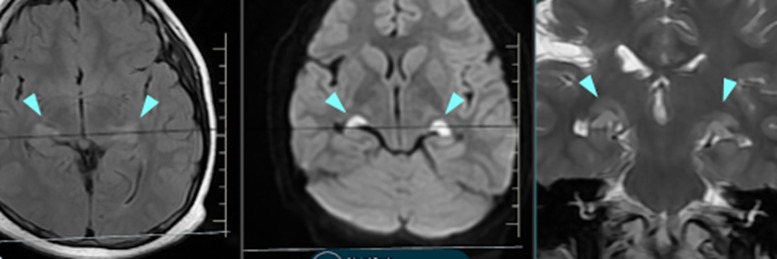
• T2/FLAIR: Bilateral well-defined hyperintensities in the lateral geniculate body regions.
• DWI/ADC: Corresponding restricted diffusion, suggesting acute cytotoxic edema.
• T1-weighted: No hemorrhage or enhancement.
• Rest of visual pathways, including optic nerves, chiasm, and occipital cortex, were normal.
________________________________________
Impression:
Isolated bilateral lateral geniculate body necrosis, most likely related to microvascular ischemia or hypoxia secondary to the systemic inflammatory response in acute pancreatitis. An extremely rare neuro-ophthalmological entity.
________________________________________
Discussion:
This case highlights a rare but diagnostically significant cause of central visual loss in a young adult. The lateral geniculate body (LGB), a thalamic relay station in the visual pathway, is vulnerable to:
• Microvascular ischemia (posterior circulation)
• Hypoxic-ischemic events
• Systemic inflammatory states
The selective vulnerability of the LGB, with normal anterior and posterior visual pathways, reinforces the need for targeted imaging in unexplained bilateral visual loss.
Bilateral LGB necrosis has been previously reported in association with sepsis, DKA, or hepatic encephalopathy—but rarely in pancreatitis.
________________________________________
Conclusion:
An important radiological diagnosis to consider in young patients with acute bilateral visual loss and systemic illness. This case underscores the value of DWI sequences and careful thalamic inspection on MRI.
________________________________________
Axial FLAIR (left), axial DWI (center), and coronal T2-weighted (right) MR images demonstrate bilateral symmetric hyperintensities (arrowheads) in the lateral geniculate bodies with restricted diffusion, consistent with acute necrosis.
Dr Ashutosh Pawale
Consultant Radiologist